
So my story started in a room such as this, at the St. Louis
national convention. My daughter was
diagnosed at 5 months and we were lucky to discover that the convention was in
our home town 2 months later. I had no
idea what to expect but it was an experience of many mixed emotions as you all
know especially since I was still in a state of shock over it all. At the St. Louis convention, we attended as
many medical sessions as we could since those were the primary issues we were
experiencing at the time. While I was
there I became very cognizant of the community’s need for straight forward
explanations of their kid’s challenges.
I saw high emotions and some speakers who struggled to give parents information
that was too scientific. This planted an
idea in my head that I could provide that sort of resource. By day I’m a human anatomy teacher and I have
a talent of explaining very difficult material in a way that people can
understand so I knew I could do that for this community. So that’s how my blog was born.

My goal in this
session today is to share with you my advocacy strategy. Now, it’s based on my experiences so it’s not
a one size fits all solution of course.
Every school or hospital has different resources or procedures BUT I
have found this form of advocacy to be very successful and hope you will too. So this presentation will be delivered in two
parts. First, as an advocate you have to
become an expert in your child. You know
your child better than anyone so you are already an expert in that regard but
knowing the whole profile and having access to professional articles and tools
will help you build valuable resources for your child’s team, in turn elevating
your role as a participant in those IEP meetings. The second phase then is sharing those
resources with the team. Having been on
both sides of an IEP table, I witnessed the whole realm of emotions that come
with them but I’ve also observed the social game and have a unique perspective on
how to navigate that.

In order to
understand that big picture to treat your whole child you should start with the
basic function of the nervous system.
When people think of the nervous system they immediately think of the
brain but our nervous system is much more complex than that. It actually begins with the sensory organs
which monitor our environment and send messages about stimuli in our
environment so we can navigate it and make decisions that keep us safe and
functional. You can probably think of a
dozen issues related to our kids’ sensory organs such as vision, hearing,
texture issues, feeding issues, attention issues… we’ll focus on a couple of
these but I want you to understand that many of your child’s behaviors are
related to this portion of the nervous pathway- gathering that
information. The issues can also extend
to how that input is interpreted. This
is a fundamental process that requires communication across the brain where we
interpret the senses and then decide on a response. WS affects a few of basic pathways in the
brain that cause our kids to interpret their environment and create a motor
output in an atypical way. Understanding this allows us to come up with creative
and effective ways to help them in the classroom. The final function is the response from the
muscles. Our kids often show muscle tone
issues and movement issues and most of those muscle issues are actually caused
by ineffective communication of the nervous system and those muscles causing
them to become overly weak or overly tense.
So this is what we’ll do for the next half hour or so, we’ll work
through these three functions and look at ways it affects a kid with WS and how
by looking at the big picture, we can help many issues at once.
 So let’s begin with
the senses. One common issue for 50% of kids
with WS is hyperopia or far sightedness.
In hyperopia, the shape of the eye causes the light to focus behind the
eye rather than hit a clear focused stream of light on the receptors of the
retina. This causes poor, blurry vision.
So let’s begin with
the senses. One common issue for 50% of kids
with WS is hyperopia or far sightedness.
In hyperopia, the shape of the eye causes the light to focus behind the
eye rather than hit a clear focused stream of light on the receptors of the
retina. This causes poor, blurry vision.
Hyperopia is a condition caused by either a flattened cornea
which is the window to the eye or due to a physically shorter eyeball and can
easily be corrected with glasses or contacts.
So you might notice your child squinting or like my Katie on the right
there, we noticed that she hated tummy time as an infant and that she tilted
her head far backwards to see things.
That was our first clue and the tummy time ended up because she couldn’t
see anything! She couldn’t pick up her
head and tilt it backwards to see the object in front of her and once we got
her to an ophthalmologist she started tolerating it better and developing
faster. If your child has poor eyesight
it will negatively affect their development because it limits the amount of
sensory input the brain receives in order to do the learning. So, it’s important to see a pediatric ophthalmologist
for testing.
The second sensory
issue we’re going to explore is hearing.
61% of our children have frequent middle ear infections, called otitis
media. You can see in the picture there,
the middle ear is the area right behind the eardrum where the ossicles or ear
bones are. The ossicles vibrate when
sound hits the ear drum and transfers that motion to the cochlea where the
sensory receptors are. Frequent ear
infections can cause delays in learning and difficulty with attention. Interestingly, our kids tend to produce
excess ear wax or have unusually narrow ear canals. My daughter’s ear canals are tilted upwards
into her middle ear which makes it difficult for the body to naturally move
that wax out. It builds up and affects
her hearing so we use ear drops, see an ear nose and throat doctor to remove it
and get a yearly pediatric audiologist assessment to make sure her hearing is functioning
properly since all those issues can directly affect her learning.

Another sensory issue that we are all familiar with that
affects 90% of those with WS throughout their life is hyperacusis. For my daughter her triggers are the leaf
blowers, vacuums and motorcycles but every kid has their own set of sound
triggers that inflicts terror and pain.
Scientists aren’t positive about what causes this issue but there are
three different theories.

The first theory is that the sound is actually
perceived as motion. The inner ear has
two regions, the vestibular apparatus made up of the semicircular canals which
monitor movement of the body and the cochlea which picks up the sound. The theory is that the vestibular
semicircular canals confuse the sound as movement, amplifying the sensory input
to the brain.
The second
theory has to do with muscle tone. Think
back to a time when you went to a loud concert or to a pep rally at
school. When you leave the venue, you
feel like sound is muffled and you speak a little too loud to people because
you can’t hear yourself. But after a
while the sound returns to normal. This
demonstrates the function of a tiny muscle in your middle ear called the tensor
tympanii whose job is to contract around the eardrum to dampen very loud sounds
and protect your hearing. The theory is
that low tone in this muscle causes it to fail to adjust to loud sounds causing
intense sound reception.
There is no real way to stop hyperacusis from happening but
we can use behavioral approaches to anticipate issues or give our kids coping
skills on how to accommodate their environment.
Things such as anticipating the sound and avoiding it such as bringing
headphones to the fireworks display or watching them from inside a room. Gradual conditioning is also very
effective. Katie was very afraid of
animated toys that move and make sounds.
So we started with just having one in the room turned off so that she
got used to the toy. Then we’d watch
youtube videos of them with the sound off so she became used to the
motion. We’d play with it when she was
out of the room so she was used to the sound but at a lower intensity and then
eventually exposed her to it. She
managed to grow out of it and moved onto other scary sounds like hair dryers
and vacuums!
So our next step
along the nervous pathway is the brain where we’ll take all this sensory information
and interpret our surroundings so we can decide on a proper response. This is called integration or association
because we’ll take that information and associate it with memories, experiences
and put all that input together like a puzzle to make sense of what is
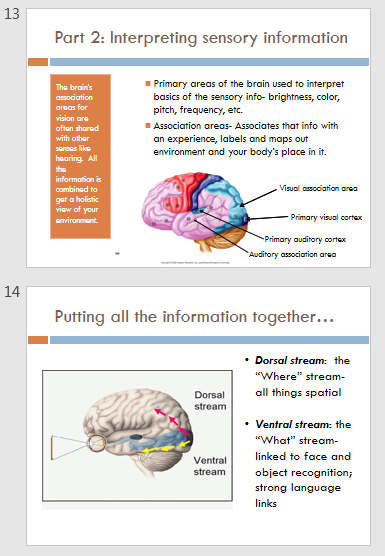
happening around us. The brain
accomplishes this with two major functional areas- primary areas and
association areas. There are primary and
association areas for all our sensory and motor functions and they are kind of
like depot stops along that pathway that put two and two together. The primary areas are our basic instincts
they are where we identify the stimulus as a bright vs dim light, the
wavelength the color the amplitude of the sound the pitch the frequency… just
basic awareness. The association areas
are where we label that as the sun and associate it with feelings, experiences
and prior knowledge.
Once we’ve labelled and figured out our surrounds we have
two major streams of information that move that nervous impulses together
toward areas of the brain that will create a response. The dorsal stream or where stream is a
nervous pathway that moves upwards towards the motor areas of the brain that
control movement. This stream is the
spatial stream where we make sense of where things are relative to one another
and it tends to be a relative weak area for those with WS.
The ventral stream moves laterally towards the temporal lobe
where our language centers are. This
stream of information illicit a verbal response and is highly associated with
speech, music and facial recognition… a strength for our kids. You can see where I’m going here, right?

So, when thinking
about WS. We can use our scientific
knowledge of how our kids think and translate that into ways we can help them
overcome their challenges. We know that
kids with WS have visuo-spatial difficulties and this is because the where or
dorsal stream has low amounts of gray matter.
The gray matter is the area of the brain where we make our decisions and
do the thinking that makes us each unique.
Since there is less development here it causes somewhat of a traffic jam
of information- they just can’t process it as effectively as the typical
person, resulting in slower activation and decision making.
Since there are
slower neural pathways in this dorsal region our kids tend to have these
difficulties- poor dexterity, slow speeds, difficulty reacting to visual
information and trouble manipulating fine motor skills. If you’ve ever watched your child try to
manipulate a coin into a slot, you’ll understand what I mean. It took Katie a very long time to accomplish
this skill and still now that she can, she still takes quite a long time to do
it and will attempt a variety of directions before she can. It also translates into self-help
issues. That same skill is used to
manipulate buttons and zippers or tying shoes for example. But knowing these issues you can also create
solutions. Until they can handle buttons,
use alternatives. Talk to teachers about
using multiple intelligences to teach them these spatial skills by tapping into
those stronger skills on the ventral pathways by using sound, music and verbal
cues.
 In addition to the
movement difficulties the integration portion of planning those movements-
called motor planning can be difficult. Also
called apraxia, this is all about predicting and planning how to move based on
senses. My daughter just recently
underwent surgery to lengthen her heel cords and the PT during her assessment
asks her to push against her hand or resist her from pushing against her foot
in order to assess her strength. You can
see my daughter’s wheels turning trying to figure out what she wants her to do.
So, we’ve approached it with a variety
of accommodations. We sing silly songs
for example, when they want my daughter to move her feet medially to put toes
together we play a game and have her “kiss” her toes and then when she wants
them to move them outwards we play “blah”.
When she does bridges we sing London bridges or when she does clam
shells we sing the shark song. All of
these little modifications help her understand how we want her to move, keeps
her engaged in the activity and improves her memory of the muscle movement
during practice at home or at later sessions.
I’ve found that when you suggest to people this approach they look at me
like I’m crazy but I just belt out my song all out of tune and go with it. Once they see that it works they pick it up
and go with it. You just have to break
the ice for them J
In addition to the
movement difficulties the integration portion of planning those movements-
called motor planning can be difficult. Also
called apraxia, this is all about predicting and planning how to move based on
senses. My daughter just recently
underwent surgery to lengthen her heel cords and the PT during her assessment
asks her to push against her hand or resist her from pushing against her foot
in order to assess her strength. You can
see my daughter’s wheels turning trying to figure out what she wants her to do.
So, we’ve approached it with a variety
of accommodations. We sing silly songs
for example, when they want my daughter to move her feet medially to put toes
together we play a game and have her “kiss” her toes and then when she wants
them to move them outwards we play “blah”.
When she does bridges we sing London bridges or when she does clam
shells we sing the shark song. All of
these little modifications help her understand how we want her to move, keeps
her engaged in the activity and improves her memory of the muscle movement
during practice at home or at later sessions.
I’ve found that when you suggest to people this approach they look at me
like I’m crazy but I just belt out my song all out of tune and go with it. Once they see that it works they pick it up
and go with it. You just have to break
the ice for them J
Now when you combine
the two difficulties- moving and space and planning on how that’s going to
work, you’ll find that nearly all our kids have difficulty with this. It’s a hallmark issue with WS and one that
will affect them in so many ways so I feel it’s an important characteristic to
discuss with your child’s therapists and teachers so they understand why your
child will have difficulty in PE or with writing. It’s part of their biology. Here I have another example with
throwing. My daughter has been working
on throwing and catching as a PT goal for about 4 years now and I don’t
anticipate that ever changing. She has trouble
seeing that ball coming to her, a sensory issue, she has to process that in her
slower where/dorsal pathway, predict where the ball will land with her motor
planning and then activate the muscles she needs to stand in the right place
and hold her hands out to catch. She has
a very slow response which typically results in her moving her hands out to
catch the ball long after it has already whizzed past her. So ways we can help? Start with slower moving objects. We practice with a balloon. It moves much more slowly so it gives her
time to process. My daughter’s PT also
works on her visual tracking to help with this skill. There is a website called Eye can learn that has simple exercises you
can use at home to help your child with visual tracking.
 The other way to
overcome these motor deficits is to tap into the strengths. Neurologists have long been fascinated with
the WS brain because we have those unique challenges paired with unique
strengths of verbal ability. Since the
where stream has a slow “two lane pathway”, the brain builds up a highway
system in the stream that allows the information to move faster resulting in a
strong verbal ventral stream. This what
stream gives our kids a strong and sometimes unique pathway and a good working
memory that is in tune with facial recognition.
It is also activated by music explaining our kid’s affinity to music.
The other way to
overcome these motor deficits is to tap into the strengths. Neurologists have long been fascinated with
the WS brain because we have those unique challenges paired with unique
strengths of verbal ability. Since the
where stream has a slow “two lane pathway”, the brain builds up a highway
system in the stream that allows the information to move faster resulting in a
strong verbal ventral stream. This what
stream gives our kids a strong and sometimes unique pathway and a good working
memory that is in tune with facial recognition.
It is also activated by music explaining our kid’s affinity to music.
The reason the
verbal stream is strong has to do with the anatomy of the neurons there. Brain
scan show that there are enlarged and more active regions in this area of the
brain. There is greater blood flow to
the hippocampus resulting in work memory strengths and there is more gray area
in the auditory regions the brain, making auditory learning a strength for our
kids.
So because our
children’s brains put more stock in this pathway we can see some of those
strengths and use them to overcome the disadvantages they experience in that
where stream. Our kids tend to have
strong memory retrieval and this stream is where our auditory areas are found
making them great auditory learners.
When they are facing tasks that require body movement from anything to
learning their letters, school work to navigating through a maze they should
combine the learning with auditory information.
This will activate more areas of their brain and keep them more engaged
in the activity.

Our kids learn differently that the typical child because of
the differences in brain matter. Very
young children with WS have delay in language development partly because they
learning and develop differently than their peers. Usually teachers search for prior knowledge
to build upon but many kids with WS rely more on their working verbal memory to
access learning so it’s important to begin lessons or supplement lessons with
listening skills. Request books on
audio, use websites that have a read aloud mode… this explains why so many of
our kids are infatuated with youtube.
They respond to the sounds and stories they hear there and process that
sound differently like we saw in the hyperacusis section.
There are some
situations where language requires the dorsal where stream and this is where
language becomes difficult for our kids.
Terms that have to do with opposites and space, size and color,
directions they all require a conceptual understanding of where something is
classified in relation to another concept.
Many of the speech therapy goals of Katie’s are centered around
understanding these concepts.
So knowing the brain
science, there are strategies you can share with care givers or use at home to
help your children tap into those verbal strengths to overcome their spatial
weaknesses. One example, you can teach
verbal reasoning. When I was in
elementary school my mom used to coach us before the big game with
visualization techniques of making the goal or imagining the muscle movement to
dive into the pool. When you watch the Olympics
you’ll see the gymnasts doing it before a vault visualizing the movements they’ll
take. This is a strategy you can teach
your children when working on spatial tasks.
Talk them through the process and help them accomplish that motor
planning they have trouble doing. By
hearing the plan they’ll have more success and gives them the skill where they
can talk through it themselves with practice to plan. The same strategy can work with
navigation. Say your child has trouble
following instructions to do a task like centers. The teacher can verbalize the instructions
before the activity or even use assistive technology on frequent tasks that
help kids follow multi step directions or navigate around their school. Provide the use of technology such as gps and
map apps for older kids and provide visual task reminders, signs or symbols to
find locations. One problem young kids
have is learning to draw shapes and later how to put those shapes together to make
a picture. For example, you’ve probably
seen that classic picture of a bike that was drawn by a person with WS where
their bike looked like a disassembled bike instead. Drawing is a very spatial task so you can
help your child by talking them through and drawing faces to learn shapes. My daughter started with drawing Mat man
which is a little person drawn with each of the shapes- circle, rectangle,
triangle, square. By connecting the
shapes to draw a person, you are tapping into the what stream in order to
accomplish a where task, making our kids more successful at it.


So when we’ve
received that visual information and made what sense that we could of it our
brain wants to send information back to the muscles of the eye in order to gain
new perspective. The message travels down
the motor pathways of the oculomotor nerve and to the muscles that surround our
eye to move our eye back and forth. That
movement is coordinated between the two eye balls to gain depth
perception. It also causes movement
within the eye in muscles that adjust the lens of the eye to better focus light
and get a clearer image.
In some children with WS especially those with hyperopia, the kids have trouble with that coordination effort resulting in estropia where the eyes aren’t perfectly aligned and one turns in or out slightly. This is a picture of my daughter when we first noticed her estropia. As a result, the two eyes are no longer looking at the same object and they get double images which further confuses the brain. If you notice this, it’s important to see an ophthalmologist immediately because if you don’t, the brain will accommodate to its surrounds which leads to bigger issues.
So if estropia
persists the brain must chose only one of those images to focus on since the input
is so confusing, so it uses sensory accommodation and begins to ignore that
weaker eye’s input. It’s just like the
little experiment we just did. You moved
your ring to a new finger. At first it
most likely made you uncomfortable. The
feeling was out of the ordinary and your body took note of it but after a while
your body decided that it wasn’t worth your attention and now it probably doesn’t
bother you. That’s what your brain does
with the weak eye information. The brain
decides its better off without the info so it turns off the input or filters it
essentially making the person accomodatively blind in the weak eye! This can cause the loss of depth perception
and overtime can become irreversible if not treated.

There are
essentially two types of estropia. This
is my daughter’s estropia a few months after we noticed it. You can see how much worse the weaker eye is
from the original photo. In this stage,
her brain began to lose interest in that sensory information and the motor
control fails causing the eye to fall in.
This can become complicated by low muscle tone or hypotonia in the
muscles. This means the nervous system
fails to keep the muscle on alert in a slightly contracted state in order to
improve and be ready for contraction. In
order to repair this, the ophthalmologist will put the children on a patching regimen
where they cover the strong eye in order to force the brain to pay attention to
the weak eye signal and keep it functional.
For some children, this will be enough to improve the eye strength. Some kids will also get glasses. Often if the child has hypotonia and far
sightedness together, the weak muscle tires and causes the eye to fatigue. By having glasses, the muscle is not worked
as hard to try and focus the image improving muscle stamina.
 There are some
situations where patching alone is not enough.
My Katie had to have surgery on her eye muscles three times. In surgery, the surgeon reattaches the
hypotonic muscle in a different place on the eye in order to shorten it and
return alignment. It’s an imprecise
surgery so it does have a high likelihood that a repeat surgery is needed but
the recovery is very fast and its’ an outpatient procedure. My daughter on her final procedure had a
botox injection where the botox temporarily paralyzes the muscle allowing it to
lengthen and stretch and then when nervous control is restored it is adjusted
to the proper alignment. This is was enough
paired with patching and the glasses to correct my daughter’s eye alignment and
her vision is restored.
There are some
situations where patching alone is not enough.
My Katie had to have surgery on her eye muscles three times. In surgery, the surgeon reattaches the
hypotonic muscle in a different place on the eye in order to shorten it and
return alignment. It’s an imprecise
surgery so it does have a high likelihood that a repeat surgery is needed but
the recovery is very fast and its’ an outpatient procedure. My daughter on her final procedure had a
botox injection where the botox temporarily paralyzes the muscle allowing it to
lengthen and stretch and then when nervous control is restored it is adjusted
to the proper alignment. This is was enough
paired with patching and the glasses to correct my daughter’s eye alignment and
her vision is restored.
So because our kids
have the stronger what or ventral stream, language eventually becomes a
strength but our kids need speech and language therapy in order to learn proper
motor output. Many of the language
strengths our kids have often cover up these weaknesses, especially as they age
so it’s not uncommon for them to lose some of their minutes to speech therapy
but there are areas that they still need help on even through adolescence. One of those is pragmatics- the art of
conversation where they listen to another person and go back and forth with information. Our kids tend to want to talk about what interests
them making friendships more difficult to maintain. With continued speech therapy, pragmatics can
be learned and our kids can have better social engagements, which they really
crave and prioritize.
More with
motor. These are pictures of my Katie at
a very young age and we are just now seeing the issues related to them. Folding in half or siting in a W are a result
of the low muscle tone that our kids tend to have and they can turn into big
problems.

When our children
are young especially they have hypotonia which is related to the motor
planning. Weak muscles are less of a
muscle issue and more of a nervous system issue. They are due to misinterpretation of the
senses and poor communication between the nerve and the muscle creating relaxed
stretched muscles with higher movement.
This creates delays in all things motor such as speech, feeding and
movement. Muscles, like the eyes are
also sensory organs. Many people don’t
realize this but we have tiny little receptors in the muscle that send back
information about where a muscle is contracted and where we are in space.
After time, the
brain begins to crave the sensory information from the muscle that it’s
missing. So, it uses muscles outside the
core in the peripheral areas of the body such as the arm and mainly the legs in
order to gain that sensory information from the proprioceptors. Early signs of this are dragging your fingers
against the wall or obstacles for balance and toe walking. When we toe walk, more specific information
is gathered from the balls and toes creating heightened awareness of balance
and our surrounding environment. It also
activates the vestibular apparatus of the inner ear amplifying information
about balance and helping us to gain more sensory info.

Toe walking can also be linking
with visual issues. Some children toe
walk to gain information that they can’t gather with their vision. With misaligned eyes, the body may get
inaccurate sense of where they are in the environment as slight forward causing
the body to want to lean forward in order to maintain balance which results in
toe walking. An ophthalmologist or optometrist
can often check for this and use prisms to correct the issue.
This overall low
tone can create big changes to the balance of muscle in the legs. They become asymmetrical. Muscles often work in pairs- when one muscle
such as the calf is in a contracted state, the opposite muscle in the shin
become relaxed. So when we have high
amounts of contraction in one muscle and overtime ignore the other, the muscles
are unevenly built creating balance and coordination issues and can lead to
joint issues.

So in the end, the
muscle aspect of this pathway is where we see the end results of all the
sensory and integration issues. By
understanding the full pathway, we can not only prevent some of the issues that
could occur such as the contractures but we can better understand our children’s
behaviors and provide sensory or integration accommodations to help them cope
or to stop problems before they require surgical intervention. For the entire pathway I might have a full
team of medical and educational professionals treating my child with myself being
the bridge between all of them in order to treat my child in full.
Which brings me to
the final portion of my presentation- how you can use all this knowledge to
become a better advocate. Because of my
background in anatomy and teaching, I’ve seen a different kind of perspective
when it comes to advocating for your child.
I found that these are the three most important aspects of my
conversations with doctors and educators and because of these conversations, I’ve
formed unique relationships with the team and created more open lines of
communication. First, I use their language
to discuss my child. When you have
conversations with a doctor, use scientific terms if you can comfortably. They pick up on this and will offer up more information
than they originally would. The same
goes with education. If you use
educational terms you can often gain more accommodations or better set the
stage to get those resources, you want.
I have an infographic that I’ve created with some of the language and
vocabulary used in this presentation that can help you in these
conversations.


Second you want to become a
resource. Offer things that the
professionals are interested in to better prepare them for their job related to
your child. Finally, the key to open up
lines of communication where you are a person who can share information will
make you a valuable part of the team.
So ways you can accomplish this are
to find professional articles which is what I write my blog posts based
on. The blog posts are for you to
understand what they say and then at the base of the page I have links to
resources used to find the info. The
professional articles listed there are great resources you can use to pass
along the information. I often print
them and give them to therapists, teachers and medical doctors. I just ask them if they’ve seen it and open
up a conversation about how it sounds like Katie’s behaviors or related to the
issues she has. For example, when it was
time for testing during Kindergarten I gave the school psychologist and speech
therapist Dr. Mervis articles on testing and speech development in order to
guide their choices.
As parent your therapists and
doctors and educators often will not communicate with each other. You are the mediator so openly share the
medical and school info with the teams so that everyone is on the same
page.


Especially for teachers, the
infographics and WSA tear away sheets are wonderful. Teachers are busy and have large caseloads so
easy to read, practical information is more likely to be read and studied than
long articles.
Another aspect of
advocacy that I’ve become hyperaware of is maintaining open communication. Sitting on both sides of the IEP table, I can
see where communication breaks down between case managers and parents when
emotion gets in the way. It really is a
social art to try and get what you want where tone and approach are so
important. You cannot just openly
request or demand things like paras or assistive technology. You have to think like a lawyer and show
evidence, set the stage for what you want.
I’ve been able to get these resources and more for my daughter without
ever requesting them. I just make a case
for it and the logical solution is to provide that resource and they have
offered it. I’m not guaranteeing success
because every district and state is different, but its’ important to understand
that work with your team should always be your first approach to an IEP.
As a teacher I have heard countless
conversations about parents who are unreasonable and I’ve found that the case
managers and teachers, like most people, who feel threatened will disconnect
from the child and become very defensive of their own decision making and
job. This is counteractive to your
overall goal of getting what is right for your child so its’ so important to
try as best as you can to remain emotionally neutral throughout the
meeting. I’m not saying you should walk
around as a brown noser but you should treat the professionals with respect because
you will in turn gain respect as well. I
make a point to thank them for their time, skills and sharing knowledge with me
so that I can better understand them and the decisions they make but in return
I’m also keeping them accountable by asking them to defend their choices in a
respectful manner. I also make it a
point to work with them instead of against them. When you offer valuable information and show
your knowledge, they will see you in a different way- as a resource that can
help them in their job rather than hinder.
When emotions get high or difficult one way, as a teacher, that I’ve
learned to reduce the charge in the room is to keep the conversation child
centered. The child is why you are there
but all too often people begin to think more about themselves if they feel
threatened which is a natural response.
If you return to phrases such as can we review how this will help my
child access the curriculum or how will this set my child up for success or how
can we help my child overcome this obstacle, you remove yourself and them from
the conversation and focus on what is important.
Some reasons why teachers and
professionals are not open to resources you want is because they aren’t
familiar or trained in them. When you
request things that are outside a teacher’s comfort zone they will often become
inflexible. I found this to be true with
my child’s special education teacher when I mentioned assistive technology. With encouragement and persistent requests
and information she became open to the idea and it ended up really transforming
her classroom by opening up the resource to many children including my
own. They say that in business you have
to pressure or present your product on average of 5 times before someone will
commit to the platform and I’ve found that in teaching this can be true as
well. As an advocate you can remain
respectful but also be offensive in this manner by repeating requests and
keeping open resources that point your teachers in the direction you want them
to go. Provide them with evidence and
resources that help make it attainable and practical.
Just like in
education, when you talk to medical professionals, the vocabulary that you use
can open of lines of communication. If
you feel comfortable, use scientific vocabulary. They will sense that you can handle more of
the details and you will learn much more about your child’s condition and tips
that can lead to better decision making.
You should also ask for medical reports from your doctors so that you
can better share the information with teachers and therapists. This will help them better understand your
child’s condition and make better plans for treatment.
The last portion, which can sometimes
be the hardest, is to ask questions. Be
open about treatment and procedures with multiple practitioners because they
often give you the best advice. When my
daughter was preparing for her surgery on her heel cords, I had a very eye
opening conversation with her cardiologist explaining the studies on anesthesia
and how to choose an anesthesiologist when you often think they are merely
assigned. He gave me advice on questions
to ask them in order to gauge their understanding of coronary stenosis and anesthesia
risk before undergoing the procedure and that I had the right to request different
anesthesiologist if I didn’t feel confident in their knowledge of WS.
Don’t rely on the internet for
details. Go there to learn more but then
ask them about what you learn and its validity.
Show them articles you find especially if they are related to your child’s
condition and are from reputable journals.
Ask about treatment options and why they aren’t recommending
others. They typically have good reasons
why they chose what they chose and can defend those decisions and if they can’t
find a second opinion!
As with medical
professionals talk is important.
Establishing a relationship as soon as possible is ideal. As soon as my daughter is placed with a
teacher or therapist, I send them information about WS. If you can get it to them before school
begins you can tap into time they have to explore that without the pressures of
the start of school prep work. As a
teacher, I always loved when parents reached out to me early and gave me tips
on how to best engage my child. It
eliminates so many trial and error days in the classroom that would occur if I
had to figure all that out on my own.
You’ll find that this open communication will often make the teacher’s
life easier and in turn they will be more likely to adjust schedules, resources
and transitions to accommodate your child because they have more power to do
that before the year begins.

Finally, the tricky
IEP meeting that stresses any parent out.
It is important to come prepared to this meeting. The parent can arguably be the most important
person in the room because no one else knows your child as well as you do. I start by creating a skills, needs and
growth sheet. All IEPs will include a
section on your child’s strengths, weaknesses and parent statement. By taking the time to write al these down
early you will not feel like you have to come up with them on the spot and you’ll
have written documentations of your wishes that will go into the folder. I often prepare these along with links or
print outs of the professional articles and infographics and send them to the
case manager about 2 weeks before the meeting.
They will be able to look this over, do the research and write better
goals because like you, time to reflect and think of these things before the
meeting will make them more throughout and developed.
Another way I prepare for the IEP
is that I become aware of what children are doing at my child’s grade level and
I write those down on paper. I reiterate
over and over throughout the meeting that I want to find ways and shape my
daughter’s goals around accessing age appropriate curriculum materials. By knowing what that curriculum looks like
you can check off skills as your case manager goes through the goals and then
if there are missing skills you find important you can request to have them
added. If the professionals don’t feel
they are developmentally appropriate, open up conversations asking them for
evidence as to why and encourage them to find ways to make it accessible such
as with technology, paraprofessionals etc.
I never outwardly ask for a para but by setting up the evidence to show
it would be a solution and an area of need, you will more likely be offered
it. It should always be centered around
your child’s needs not what the general population of WS children need. I have the professional opinion that every
child with WS is uniquely different. Because
special education is tailored toward your child you must be mindful of what is
right for your child and aim for that. You
should be knowledgeable of the options and flexible to try new things. If you show those traits your team often will
as well and you will form a strong working relationship. Finally show gratitude when your team is
flexible, uses your resources and shows a desire to go above and beyond. It will only make your relationship stronger
for future problem solving and negotiations.
Resources to share with experts or use at home:
- Infographics- terms for parent advocacy and visual spatial strategies for teachers: https://drive.google.com/drive/folders/0B3vIN5__SQqLVU1xZGtqYThPdVU
- Practical guide to helping your child overcome anxiety and more
- Visually guided step decent in children with WS
- Neural mechanisms in WS
- Visual spatial deficits related to WS genetics article
- Spatial deficits in children with WS academic article by Bellugi
- Assessment of intellectual and visual spatial abilities in WS
- Hyperacusis in Williams syndrome
- Hyperacusis- fears, awareness and attraction professional article
- Oromotor praxis in WS
- Therapy and educational sample goals sheet from the WSA
- Parent and educator strategies for students with WS
No comments:
Post a Comment